

 has defined a vision that breaks the issue down into “five steps”; more protection for the most vulnerable; improve infrastructure, reduce food waste, grow a wider variety of crops and focus on child nutrition. As we discussed the others, today we bring our attention on child nutrition.){kind=link}
To “reduce hunger in the world,” the World Food Program (WFO) has defined a vision that breaks the issue down into “five steps”; more protection for the most vulnerable; improve infrastructure, reduce food waste, grow a wider variety of crops and focus on child nutrition. As we discussed the others, today we bring our attention on child nutrition.
The emphasis on child nutrition is simply providing good health and nutrition for the first 1,000 days of a child, which is critical to preventing stunting and promoting healthy development. Stunting is the impaired growth and development that children experience poor nutrition, repeated infection, and inadequate psychosocial stimulation. Children are defined as stunted if their height-for-age is more than two standard deviations below the WHO Child Growth Standards median. In simple terms, delayed growth refers to an inability to achieve its full growth potential.
Stunting in early life, especially in the first 1000 days from conception until the age of two – impaired growth has adverse functional consequences on a child growth. Some of those effects include poor cognition and educational performance, low adult wages, and lost productivity. Also, when accompanied by excessive weight gain later in childhood, an increased risk of nutrition-related chronic diseases in adult life. Linear early childhood growth is an important marker of healthy growth due to its association with risk of morbidity and mortality, non-communicable diseases at the end of life, and learning capacity and productivity. Further, it is closely connected to child development in many filed, including cognitive, language and sensory-motor abilities.
It is important to note that stunting is largely irreversible: a child cannot recover their height in the same way as they can gain weight. Stunted children get sick more often, miss out on learning opportunities, do less well in school, and grow up economically poor, and more likely to suffer from chronic diseases. This affects badly to a country and its economic growth in the long run.

Figure 1. Three faces of malnutrition, 2021
Stunting is the most widespread form of child malnutrition, with an estimated 149 million children worldwide by 2021 (Figure 1). Although the number is a little lower than it was ten years ago, it is still significantly higher. The average stunting value for the world is close to 23 percent for the children. As a region of South Asia show the highest percentage of stunting, 35.8 percent for children under five years of age (figure 2). Eastern and Southern Africa is second with 34.5 percent. In general, we see that Africa
and Asia are facing a serious problem. The three countries with the largest number of stunted children are India (46.6 million), Nigeria (13.9 million) and Pakistan (10.7 million). Interestingly, the three countries with the largest number of children that are wasted are almost the same – India (25.5 million) and Nigeria (3.4 million) but also Indonesia (3.3 million). Wasting is defined as weight loss for height. It often indicates recent and severe weight loss, although it may also persist over a long period of time. This usually occurs when a person has had inadequate quality and quantity of food and/or has had frequent or prolonged illnesses. Rising food prices, droughts, floods and other climatic impacts, as well as other food production and distribution mechanisms, all have an impact on the short- and long-term impacts of child malnutrition. Thus, comprehensive, efficient, and effective food programs should be launched to overcome child malnutrition and help affected countries achieve economic growth.
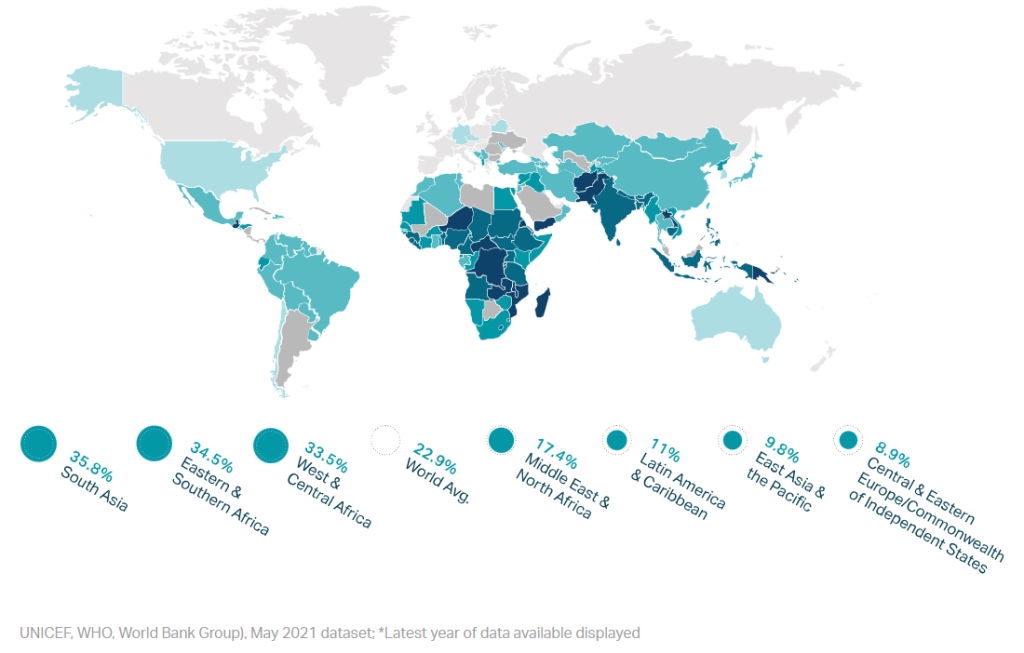
Figure 2. Percentage of children under the age of five who are stunted.
What can be done to improve child nutrition?
Based on the different activities carried out and their success, it suggests different programs which can be launched to combat child malnutrition i.e., to avoid stunting and wasting. Some of them are community programs to ensure household access to proper sanitation, clean water supply and diversified foods, poverty reduction support for families in need, education on how to feed young children and protect them from infection, and adequate, accessible health services to prevent and treat infections. Such programs are being conducted around the world where child nutrition is very important. Some programs have also improved outcomes.
For example, in Maharashtra, India, the prevalence of stunting was reduced by 16 percent in seven years through delivering proven community level interventions, in a focused and equal way, equipping frontline health workers to deliver nutrition services and behavior change communication activities (Livelihood & Food Security Fund). Bangladesh has reduced stunting by 1.4 percent a year since 1997: the key drivers of this are improvements in household assets, parental education, sanitation coverage, health care use and nutritional services. Vietnam has extended maternity leave to six months and banned the advertising of breast-milk substitutes, which are known to cause a decrease in exclusive breastfeeding rates. This policy action was reinforced by public awareness campaigns to promote key messages and give credibility to the work of health workers. The success depends on the community level support to mothers a s well. Brazil reports amazing results with increasing the length of time for breastfeeding. Brazil could reduce stunting from 37 per cent to 7 per cent in 30 years by increasing length of time breastfeeding from 2.5 months to 14 months. Mexico reports gains reducing stunting by 10 percent, with a “cash transfer combined with nutrition and health education, micronutrient supplementation”.
Increasing economic growth in a country is important to reduce stunting and child malnutrition. For example, Cambodia has experienced rapid socioeconomic development since international peace agreements, opening itself to an open market economy. As a consequence, stunting among children declined from 49.3 percent in 2000 to 39.0 percent in 2010, due to increased household wealth, increased access to sanitation facilities, improved maternal and paternal education levels, longer intervals between births, and decreased prevalence of maternal tobacco use. A study conducted in Oman found that the size of children increased with the increase in the education of mothers. An urban agricultural program in Ecuador shows a reduced growth retardation of children as well. There are many others like community-based nutrition education and promotion platforms and energy and protein supplements for women that have produced positive and significant results.
All of us must be involved in the battle of child nutrition. We all have different ways of doing it. Some of us can educate others and give them more information about child nutrition, food nutrition and other health issues. Others can directly contribute to agricultural activities that help increase food availability worldwide. There are NGOs and other governmental programs that work on child nutrition, and some of us can give for them. Furthermore, we can be part of the program by reducing our erroneous behaviors associated with the production, distribution, storage, cooking, and consumption of food.